It all began when patient zero was identified with COVID-19 on 31st December, 2019, in Wuhan, China. Since then, life all over the world has changed. All the little things that are taken for granted – from stepping outside for a cup of tea to touching one’s face – are now a threat to oneself. Compared to the fatal numbers of many other countries, there are now 5,913 [corona.gov.bd, 27th April] confirmed coronavirus cases in Bangladesh. But a potential for a surge remains unless we adopt measures, and prepare for a possibly catastrophic future.
COVID-19 is not only a public health or medical issue; it requires a multidisciplinary planning and approach. The outbreak and spread of the virus challenges not only the virological and epidemiological fields but also requires the critical intervention of spatial planning. Urban systems and deadly diseases have maintained a correlation that functions in parallel during and after the outbreak. Nineteenth-century cholera pandemics in Europe resulted in developments of water and sewage systems. In 1854, British physician John Snow used geographic mapping to locate a cholera outbreak in London that led to the saving of many lives. Even though scientists at that time did not fully understand what caused the yellow fever outbreak in 1793, Philadelphia began building one of America’s first water treatment plants after the fever subsided.
Many of the successful measures taken by some countries to reduce the spread of COVID-19, as well as to bring down the number of deaths, are based on a collaborative and multi-agency action.
COVID-19 may gradually create a substantial change in the urban system once it de-escalates. But while it is still in progress, it is also extremely crucial to have a better assessment of successful strategies in various countries so that we can identify and analyse possible measures that can operate in our own context.
Most virus-affected western countries have imposed a temporary lockdown, or a slowdown, on their people to ensure fewer gatherings so that the spread of the virus is slowed, and the surge on hospitals is levelled. Until 14th April, Europe still remained as the core of the COVID-19 pandemic. Currently, on a global scale, the United States has the highest infection rate, as well deaths. While these countries have imposed lockdowns and closed borders, they still have had a difficult time keeping the numbers down.
On the other hand, New Zealand seems to have managed in containing the outbreak before it ever had a chance to begin. Some East Asian countries are also managing in an effective way. Vietnam, for instance, has had fewer cases with no death count so far. With the motto of ‘proactiveness and consistency throughout the response’, Vietnam is one of the first countries to have sealed down neighbourhoods when workers started coming back from China after Chinese New Year. They also put most emphasis to build awareness in their own cultural way of dancing, singing, and making short animations.
Of all countries, South Korea, Singapore, China, and Taiwan have taken effective strategic measures at the right time, and have been largely successful to slow down the spread of coronavirus compared to many developed countries. It is known that the novel coronavirus (SARS-CoV-2) has a genetic relationship with SARS-CoV that caused an outbreak during 2002-2004, mostly in Eastern Asia. South Korea, Singapore, China and Taiwan took a lot of lessons from that epidemic, and started taking precautions to tackle novel coronavirus long before they tracked down the first patient in the region.
Since the antidotes or vaccines for novel coronavirus are still in the pipeline, the East Asian countries cited here used both pragmatic and high tech systems. Taiwan used prevention and policies to reduce the infection rate. China taught us the importance of preparedness to prevent and control infectious disease outbreak with technology and pragmatic systems. On the other hand, South Korea emphasised more on isolating the patients and building awareness among its people using the social media platform. The main focus of Singapore was to track the virus-affected people, and isolate the virus-free people from the affected ones by keeping the latter in hospitals until they recover.
Researchers at Bengal Institute looked at Taiwan, Zhejiang Province and Hangzhou in China, South Korea and Singapore for a close look at the strategies each country developed and implemented to fight against COVID-19. We, in Bangladesh, can learn from these strategies in how to devise our own successful measures. In two parts, we present a comparison of successful strategies of the four countries, and the measures that we can take. Here we present a comparison:
Taiwan: Taiwan implemented a 124-point action plan to keep the death rate to less than 2% of the confirmed cases. The country was also very strict about border control and screening. Government policies to isolate people and mandate on the mask export, and fixing selling price and local production proved effective for public health.

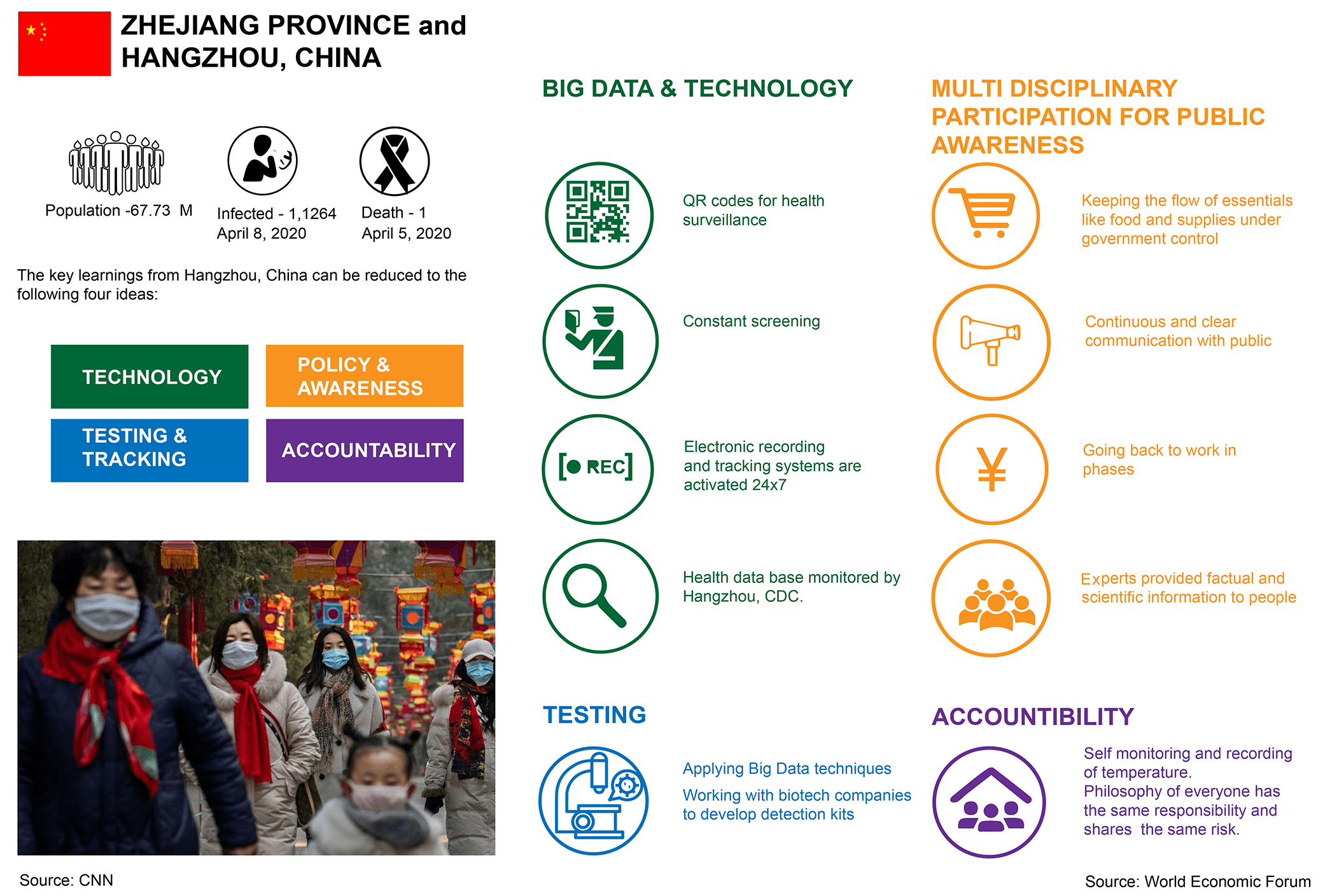
Hangzhou, China: Hangzhou is the capital city of Zhejiang Province, about 1,000 miles away from Wuhan, the epicentre of COVID-19. The city was cautious the very moment a pandemic broke out in Wuhan, and went into a lockdown to prevent the infection. China’s use of technology helped management facilities to isolate, monitor and treat positive cases with accuracy. With constant tracking there was a breach of privacy but identification of infected cases was prompt and efficient. This also reduced the contamination in clusters.
South Korea: Having conducted over 15,000 tests daily, South Korea also maintains an expansive and organised texting system. This allows the country to completely isolate the patients from the virus-free people. With the help of apps, the authority keeps track of the patient’s whereabouts, and also lets people know who may have come in contact with the patient in recent times based on their recent locations. The idea is to identify and isolate every single person who may come closer to the affected person.

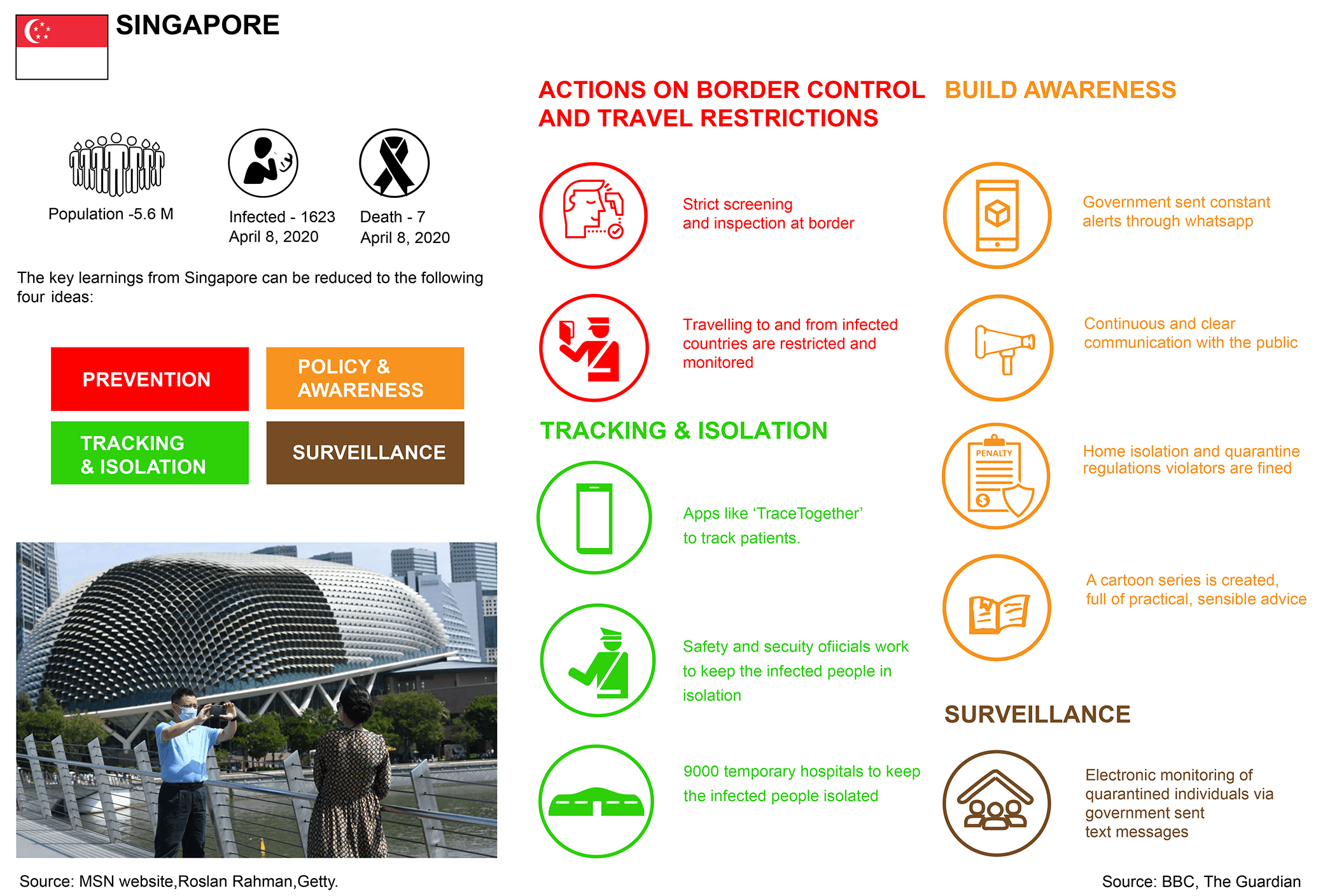
Singapore: The early preparation taken by the authority has been in favour of Singapore. It relied on tracking the affected people using the vast network of social media, apps and text messages. Over 9000 temporary health clinics have been established to keep the patients isolated. The goal is to keep the affected people completely separated in temporary clinics from the virus free community, and to make sure no transmission takes place through them.
As there is no universal antidote yet, COVID-19 is here to stay for a long haul. Even when the virus subsides, there is a danger of a second wave, and a greater economic and social pandemonium.
From Madrid to Mumbai, and from Detroit to Dhaka, at present, no place on earth is immune from the reach of the coronavirus. But the outbreak, spread and subsidence of coronavirus cases vary from region to region. In part 1 of this study, we looked at four countries with a high success rate in managing the virus. In this part, we identify and analyse possible schemes that can be put in place in Bangladesh, and can be both effective and fitting to our social and economic context. The most crucial thing to consider is how to gradually regularise everyday public activities with proper safety measures utilising the best of the resources we have. Considering all variables remain constant, it is possible to keep the infection rate low with timely policies and pragmatic systems. For example, a community of 50,000 Chinese people in Prato, Italy, who went under lockdown even three weeks before Italy’s first infection, kept their rate less than 50% than the whole of Italy.
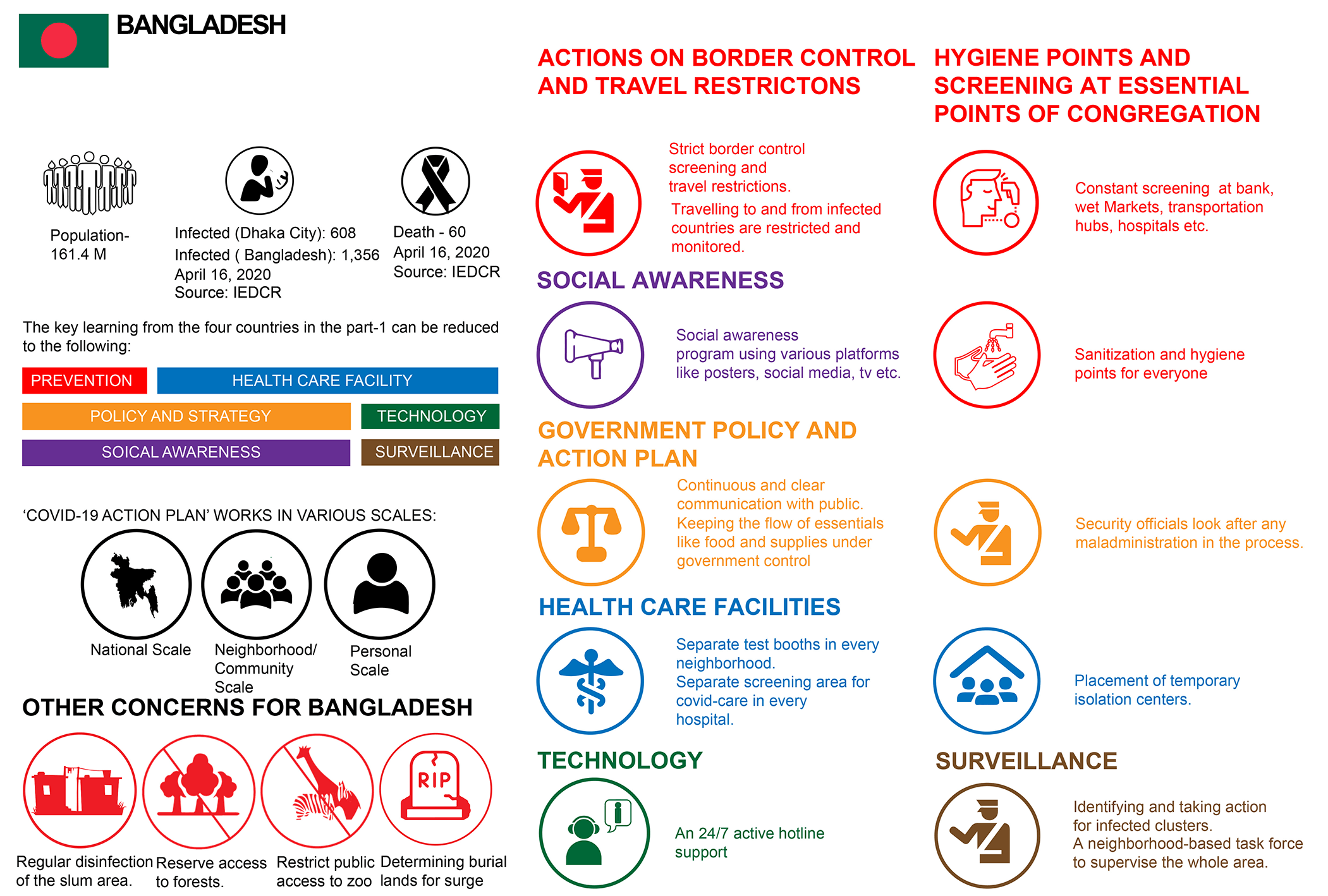
As the virus slowly spreads its insidious tentacles, Bangladesh stands on a vulnerable precipice. With a high transmission rate, especially in densely populated places, it becomes a challenge to tame the numbers of people getting infected.
Many actions are already being taken in Bangladesh. The country has been under lockdown since 26th March, that involves suspending all modes of inter-city transport and shutting down of institutions, offices and businesses. Testing for COVID-19 infection is now being conducted in 14 labs: 9 in Dhaka and 5 in different districts. Private groups have started setting up temporary hospitals around Dhaka to accommodate the vast number of infected people. Few awareness campaigns are already in circulation on social media, television and newspapers. While these developments are crucial to tackle this crisis, the outbreak requires formulating a ‘COVID-19 Management Action Plan’ from the national to the neighbourhood scale.
Besides funds and resources, and well-trained personnel who can deal with the virus, Bangladesh faces other challenges, such as, shortage in approved testing centres and health treatment facilities, lack in prevention and hygiene awareness and social inequity. This could become more of a trial if we are to face a surge in both virus cases and hospitalisations. Researchers from Bengal Institute believe that we can still keep the death rate low with a choreographed community and government support.
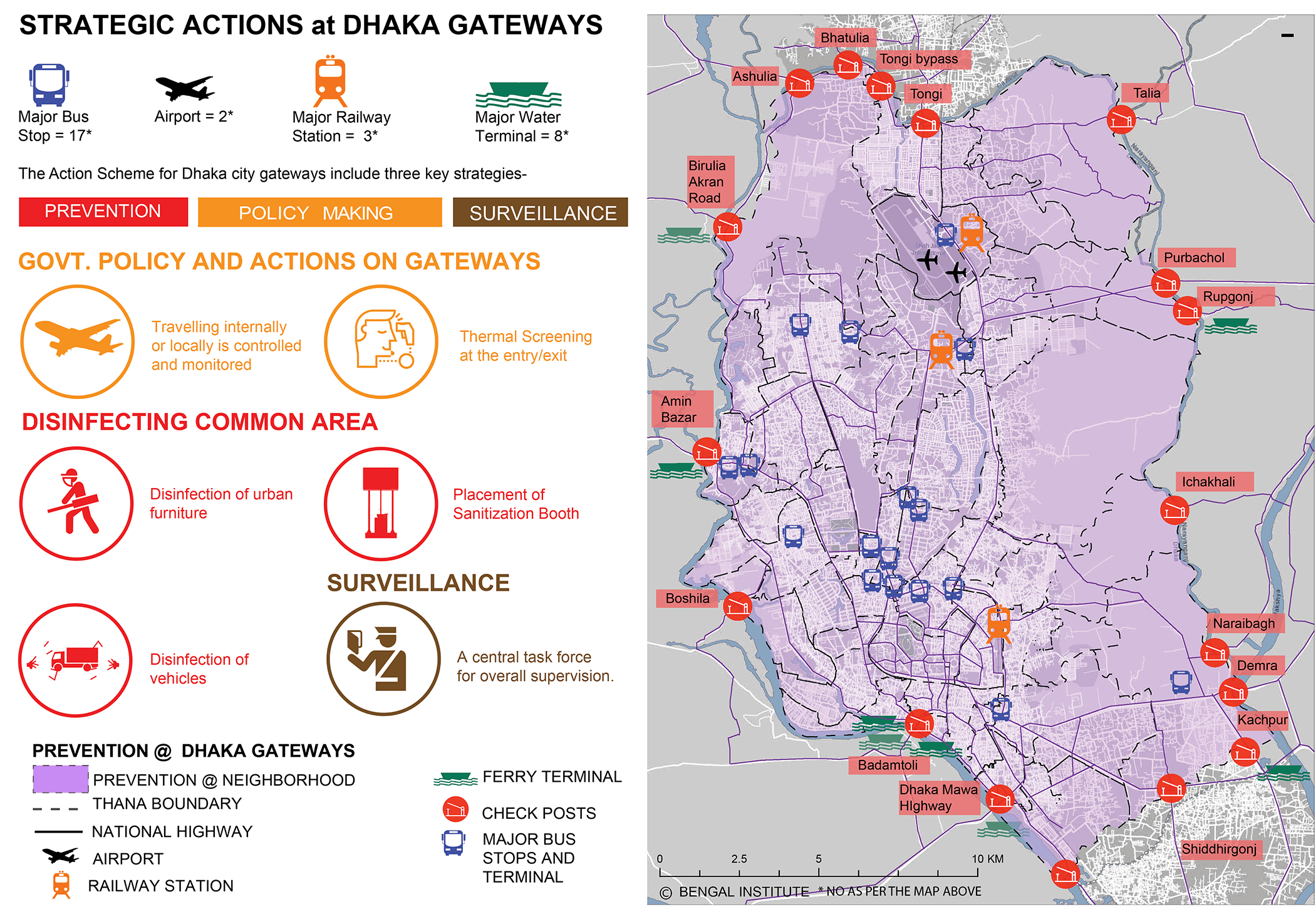
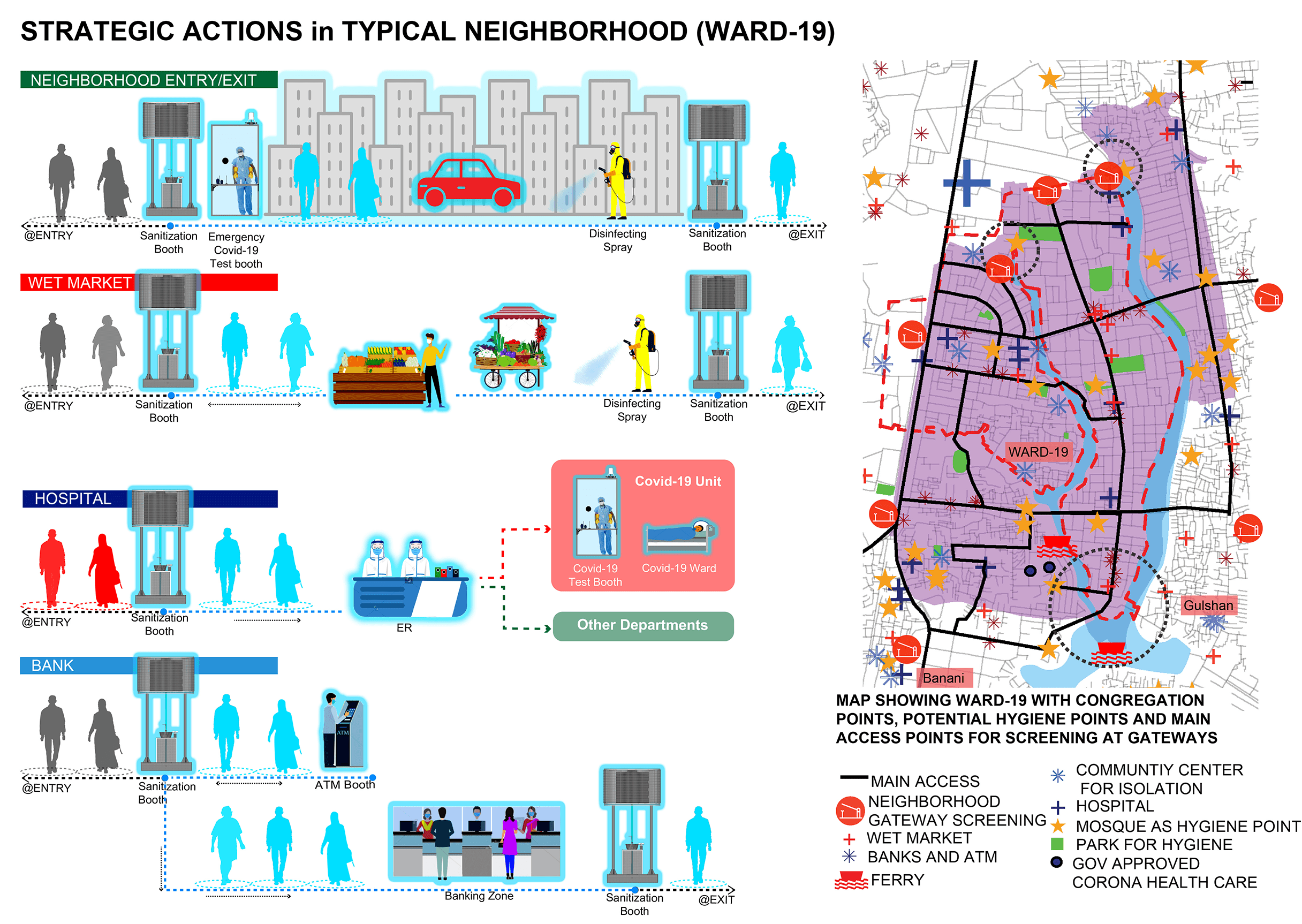
The show must certainly go on. Even during a pandemic, the need for basic amenities and services does not vanish. Essential services such as wet markets and groceries, banks, ATM booths and regular hospitals need to be accessed by people. Additional health screening and/or sanitising should be a priority for such points of congregation.
At a national scale, modes of transportation and mobility are gateways for future infections. At present, there are 18 national highway gateways to Dhaka city. Besides, there are airports, private helipads, train stations and bus stations connecting the metropolis to the rest of Bangladesh and the world. Strict border control and inspection at gateways cut down a lot of foreign-borne contamination.
Prevention measures can certainly begin from the national scale, but they can be applied to three key scalar conditions: city or town, neighbourhood and health care facilities. For each city or town administration, action measures may be taken to locate the critical nodes of the city. At those nodes – such as gateways and entry points – strict screening may be applied. Travel restrictions and control may be applied at city and even at neighbourhood level, that can be eased only with the lowering of transmission and hospitalisation rate. A strategic plan should be in place for establishing temporary hospitals, where care must be taken regarding the site, emergency transportation facilities, water electricity access and key staff. Infected neighbourhoods and areas should be under surveillance of city and town administration along with community participation. To make a multi-scalar plan work, it is critical to maintain a close overall supervision by a central task force.
At the metropolitan scale, such as with Dhaka, decisive public health and hygiene actions come with a demand for logistics. A surge may not only require setting up of more health facility centres but sadly burial grounds. In Dhaka city, there are at least 247 mosques and 22 parks under renovation. With supply of water, some of these places can be potential ‘hubs for hygiene’.
At the neighbourhood scale, public places can be mapped both for the facilitation of regulated food and wet markets, and setting up field hospitals if needed. Such mapping is important as amenities and facilities are not equal for every neighbourhood. Points of crowding can also be mapped and measures taken for regulating gathering, as well as setting up sanitisation booths, especially for pedestrians, rickshaw pullers and certain vendors. Such booths may also be set up at the entry and exit of main mohollas and urban blocks. Houses and other buildings may be sanitised regularly. Awareness momentum should be maintained through posters, banners and leaflets.
The business-as-usual health care and hospitalisation facilities will not work in the case of an infectious disease as COVID-19. Segregation of virus affected patients from the non-infected patients is as critical as hospitalisation. Even services such as testing and checkup for coronavirus should be conducted in clearly designated areas.
While surveillance is always a tricky practice, it is essential to track and trace infected people and isolate them from the normal group. Apps may be used to trace infected people and their movement patterns. At the end of the day, personal awareness remains the starting point of prevention against COVID-19. The more awareness we can create, the more we can prevent infections.
Writings and illustrations by: Sabiha Haque and Samira Marzia.
Research facilitated by: Nusrat Sumaiya.
Originally published on The Daily Star. Short link to this page for easy sharing: http://bit.ly/ConfrontingCovid
For everything else on Bengal Institute’s COVID-19 efforts click: 
